A personal reflection on the journey to eliminating trachoma as a public health problem in Australia by Professor Hugh Taylor
As a university student, I once drove through the Ophthalmia Range, named by Ernst Giles after he caught trachoma there in 1876. Later I learnt about Sandy Blight Junction, where Len Beadell caught trachoma in 1960.
Australia’s geography is, in some ways, marked by trachoma.
As an ophthalmology trainee, I learnt a little more about the disease. Trachoma was the reason many eye hospitals around the world were established, including the Royal Victorian Eye and Ear Hospital in 1866.
Yet by 1909, Sir James Barrett noted there were no cases of active trachoma in Melbourne. To teach students, he had to bring patients in from Gippsland or the Goulburn Valley.
During my own training, I saw only one or two cases of old trachoma in elderly rural patients.
Trachoma had disappeared - or so I thought.
In 1976, I began working with Fred Hollows on the National Trachoma and Eye Health Program.
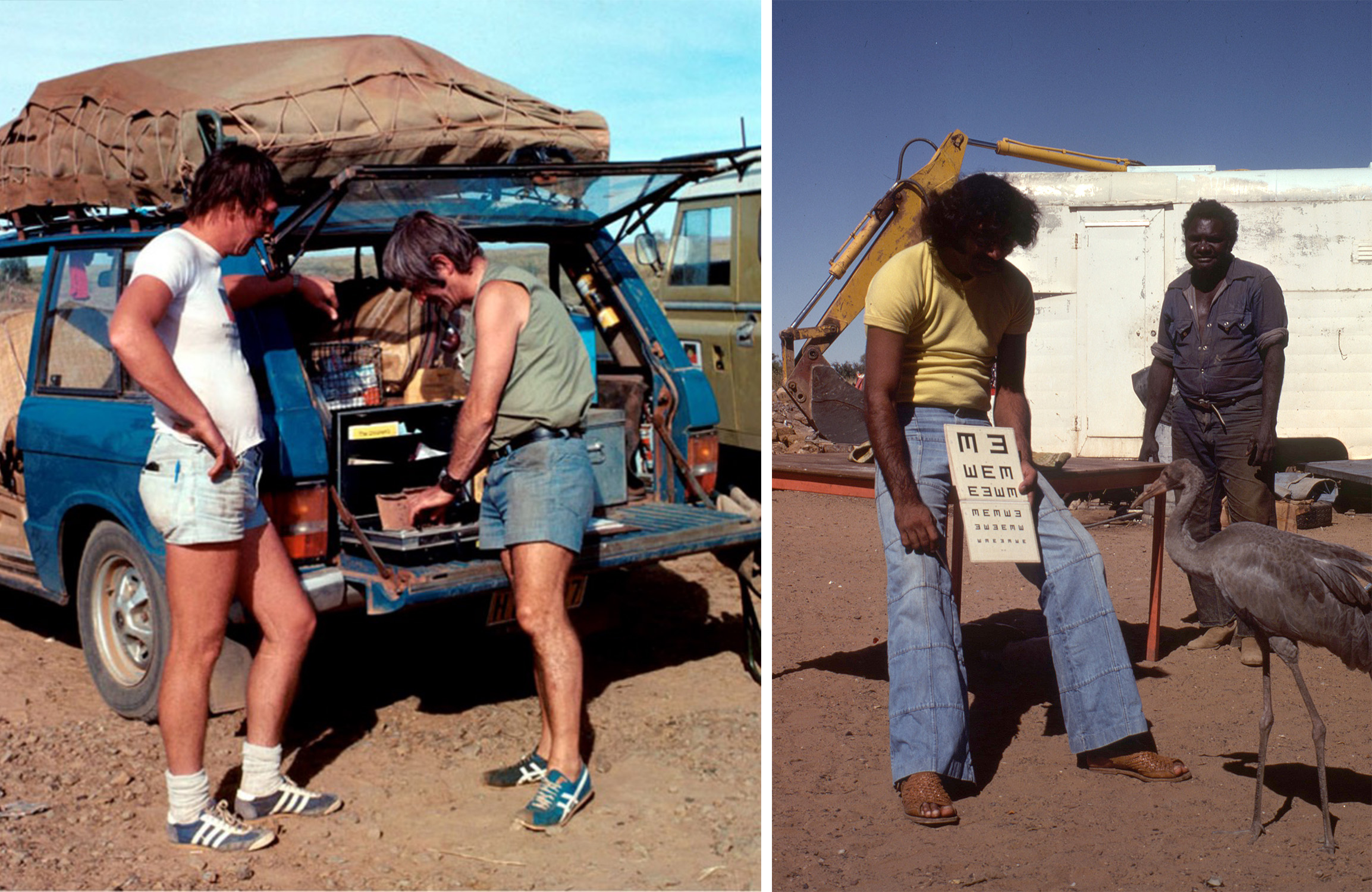
L: Hugh Taylor and Fred Hollows consult at the back of Fred's 'Blue Berry', Kimberley, Western Australia, 1977; R: Trevor Buzzacott testing vision during the National Trachoma and Eye Health Program, Kimberley, Western Australia, 1977
We examined over 60,000 Aboriginal and Torres Strait Islander people and almost 40,000 non-Indigenous Australians. Across the country, around 17% of Aboriginal and Torres Strait Islander children aged 15 years or less had active trachoma.
In some rural areas, rates were around 3%. In more remote areas, they reached as high as 64%.
Community-wide antibiotic treatment was introduced, trichiasis surgery was performed where needed, and jurisdictional teams were established.
But progress was not immediate.
When I returned to a remote community I had visited in 1977, I found that, 20 years later, the prevalence of active trachoma in children remained at 72%.
While working at Johns Hopkins University, our animal model studies showed the importance of repeated infection.
Later field studies confirmed that it may take 150 to 200 episodes of reinfection for enough damage to occur to cause the scarring that leads to blindness.

Hugh Taylor examining a child for trachoma, Katherine Region, Northern Territory, 2008.
These studies also showed the importance of facial cleanliness — the most effective way to reduce transmission from one child to another.
With improved surgical techniques and the development of azithromycin, the World Health Organization launched the global initiative GET 2020, based on the SAFE strategy:
- Surgery
- Antibiotics
- Facial cleanliness
- Environmental improvement
In Australia, after extensive advocacy, the Australian Government committed in the mid-2000s to a coordinated national approach to eliminate trachoma among Aboriginal and Torres Strait Islander people.
- Annual screening and surveillance
- Widespread antibiotic distribution (including azithromycin)
- Investment in health promotion
- Strong partnerships with Aboriginal Community Controlled Health Organisations (ACCHOs) and communities
- Local jurisdictional teams leading implementation
Annual surveillance data were collected and reported nationally, providing a clear picture of progress over time through the National Trachoma Surveillance and Reporting Unit, initially based at the University of Melbourne and later at the Kirby Institute.

L: Hugh Taylor with Liz Dax and the Minum Barreng team, Laramba, Northern Territory, 2019; Hugh Taylor with Trevor Buzzacott, Anangu Pitjantjatjara Yankunytjatjara Lands, South Australia, 2019

Hugh Taylor interviewed with Melbourne Football Club, Ltyentye Apurte (Santa Teresa), Northern Territory, 2019
Health promotion played a critical role.
Messages about clean faces were carried through posters, radio and television, school programs, murals, and community events. With the support of the Melbourne Football Club, these messages were also promoted through sporting activities.
At the centre of these efforts was Milpa the Goanna, with a simple and powerful message:
There was also a strong focus on ensuring access to safe and functional washing facilities - including prompt repairs and ongoing maintenance.
But an important lesson emerged.
In communities where trachoma had disappeared, around 90% of children across all age groups had clean faces.
In communities where trachoma remained:
- Only around 30% of younger children (1–4 years) had clean faces
- Around 60% of children aged 5–9 years had clean faces
- Around 90% of older children had clean faces
These children lived in the same houses and used the same facilities. The difference was not just the ‘hardware’ (safe, functional washing facilities), it was also the ‘software’ - including behaviours, routines, and support within families.
Younger children needed support from family members and carers to keep their faces clean until they were old enough to do it themselves.
Over time, with sustained effort, strong community leadership, and coordinated action, rates of trachoma steadily declined.

L: Lesley Martin showing how to clean faces, Yuendumu, Northern Territory, 2022; R: Milpa on the football field with kids in Yuendumu, Northern Territory, 2013
By the end of 2025, Australia was able to submit a dossier to the WHO seeking validation that it had achieved the elimination of trachoma as a public health problem.
This is a remarkable achievement, and one that belongs to many. To the communities, to the health workers, to the organisations, and to all those who have contributed over many years.
The work now is to ensure that trachoma does not return. This will require ongoing monitoring of any potential recrudescence, the continued detection and referral of trichiasis, and access to treatment where needed. Most importantly, it will require maintaining high levels of facial cleanliness and ensuring that safe and functional washing facilities remain available in communities.
Looking back over this work, one of the most important lessons has been the role of communities themselves. As we look to the future, this leadership remains central.