Project Summary
Inequalities are evident in early childhood caries rates with the socially disadvantaged experiencing greater burden of disease, including families with a refugee and migrant background. The Teeth Tales research study began in 2006 due to community concerns for the oral health of children from a refugee or migrant background residing in the Moreland and Hume local government areas (LGAs) of Melbourne. Our preliminary research showed that oral health programs and services were not reaching refugee and migrant communities who are at an increased risk of poor oral health. Through a qualitative study conducted in 2006 – 2009 the sociocultural influences on oral health were explored. The findings from this study suggested that poor oral health may be due to their migration experience and difficulties accessing services; there are socio-cultural differences in relation to child oral health knowledge, beliefs and practices; and oral health promotion needs to incorporate the discussion of traditional oral health practices.
Based on the findings from this qualitative study the next phase of Teeth Tales was designed and piloted to explore the implementation of a community based child oral health promotion intervention for children from a migrant and refugee background. The pilot study, conducted in 2011 in the inner city suburb of North Richmond, aimed to determine if the model was feasible and acceptable in a culturally diverse community setting. Trained peer educators recruited families from the Vietnamese, Sudanese and Oromo communities to be involved in the intervention. Learnings from the pilot phase provided valuable information to inform modifications for the subsequent trial; particularly relating to the inclusion of cultural organisations as partners; altered study design and recruitment processes and the consideration of the relevance of the program to newly-arrived migrant communities due to resettlement issues. It was then ready for a larger scale exploratory trial.
Teeth Tales is a research study that adopted a culturally competent, community participatory approach to child oral health promotion. Families from an Iraqi, Lebanese or Pakistani background with children aged 1– 4 years, residing in metropolitan Melbourne, were invited by trained peer educators from their respective communities to participate in the trial using snowball and purposive sampling techniques. Moreland, a culturally diverse, inner-urban metropolitan area of Melbourne, was chosen as the intervention site. The intervention comprised of peer educator led community oral health education sessions, with the intent to improve oral health through increased oral health related knowledge, confidence and the adoption of positive oral health behaviours. The intervention also endeavoured to enhance the cultural competence of services for refugee and migrant families, including family and dental services, through a Cultural Competence Organisational Review (CORe) for participating community health services and local government. A total of 688 children from 521 families from a Lebanese, Iraqi and Pakistani background living in metropolitan Melbourne were recruited into the study.
Teeth Tales Partners
The Teeth Tales study has been a 9 year project led by The University of Melbourne and Merri Community Health Services (MCHS) in partnership with Dental Health Services Victoria, Moreland City Council, Arabic Welfare, Victorian Arabic Social Services, Pakistani Australia Association of Melbourne, The Centre for Culture, Ethnicity and Health, North Richmond Community Health and Yarra City Council.
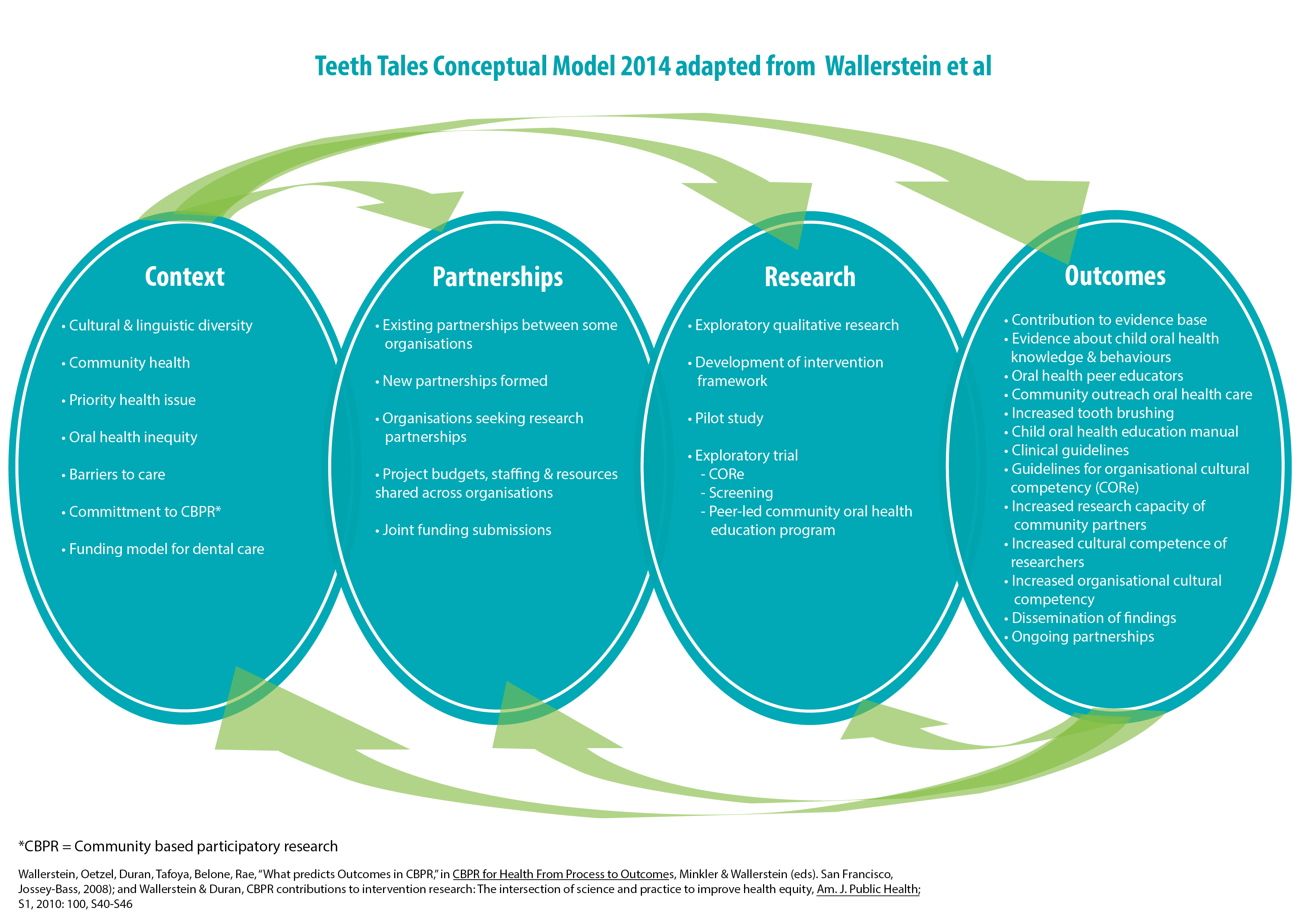
A conceptual model for the Teeth Tales study was developed by the project partners in 2014 based on the Wallerstein et al conceptual logic model of community based participatory research (CBPR). This model is a concise way to present the multiple facets of the Teeth Tales study and also to aid in dissemination of the project findings. This CBPR conceptual model can be applied at any stage of participatory research.
Teeth Tales Showcase
This project was successfully completed in 2014. A showcase of the study findings and outcomes was conducted on the 23rd of October 2014. Read about the project showcase here.
Media coverage
- 'Teeth Tales tells a story', VOICE vol 10: 11, 2014.
- 'At last, project with Teeth' Moreland Leader Newspaper, 3rd November 2014, page 3
Key Papers to date
- Gibbs L, Waters E, Christian B, Gold L, Young D, de Silva A, Calache H, Gussy M, Watt R, Riggs E, Tadic M, Pradel V, Hall M, Gondal I, Moore L. Teeth Tales - A community based child oral health promotion trial with migrant families in Australia. BMJ Open. 2015;5:e007321. doi: 10.1136/bmjopen-2014-007321
- Christian B, Young D, Gibbs L, de Silva A, Gold L, Riggs E, Calache H, Tadic M, Hall M, Moore L, Waters E. Exploring child dental service use among migrant families in Metropolitan Melbourne. Australian Dental Journal. 2015. 60(2): 200-204
- Gibbs L, Waters E, de Silva A, Riggs E, Moore L, Armit C, Johnson B, Morris M, Calache H, Gussy M, Young D, Tadic M, Christian B, Gondal I, Watt R, Pradel V, Truong M, Gold L. An exploratory trial implementing a community based child oral health promotion intervention for Australian families from refugee and migrant backgrounds: A protocol paper for Teeth Tales. BMJ Open. 2014;4:e004260. 10.1136/bmjopen-2013-004260
- Riggs E, Gussy M, Gibbs L, van Gemert C, Waters E, Priest N, Watt R, Renzaho A, Kilpatrick N. Assessing the cultural competence of oral health research conducted with migrant children. Community Dentistry and Oral Epidemiology 2014 42:1; 43–52
- Riggs E, Gibbs L, Kilpatrick N, Gussy M, van Gemert C, Ali S, Waters E. Breaking down the barriers: A qualitative study to understand child oral health in refugee and migrant communities in Australia. Ethnicity and Health. 2014. doi: 10.1080/13557858.2014.907391
- Riggs E, Gussy M, Gibbs L, van Gemert C, Waters E, Kilpatrick N. Hard to reach communities or hard to access services? Migrant mothers' experiences of dental services. Australian Dental Journal. 2014; 59: 201-207
- Riggs E, van Gemert C, Gussy M, Waters E, Kilpatrick N. Reflections on cultural diversity in oral health promotion and prevention. Global Health Promotion. 2012; 19(1): 60-63
- Gibbs L, Gold L, Kulkens M, Riggs E, Gemert CV & Waters E. Are the benefits of a community-based participatory approach to public health research worth the costs? Just Policy. 2008; 47: 52-59.
- Waters E, Gibbs L, Renzaho A, Riggs E, Kulkens M, Priest N. Increasing Cultural Competence in Public Health and Health Promotion. In Heggenhougen K (ed) International Encyclopedia of Public Health. Elsevier Inc., Oxford UK. 2008, pp38-44.
- Gibbs L, Waters E, Renzaho A, Kulkens M (2007) Moving towards increased cultural competency in public health research. In A. Williamson & R. DeSouza (eds) Researching with communities: Grounded perspectives on engaging communities in research. London: Muddy Creek Press, pp339-355.
Final Outcomes
1. Impact of research on health outcomes
The follow up measures in the Teeth Tales trial showed improved child oral hygiene, improved parent knowledge of tooth brushing technique and increased knowledge of the role of fluoride in the water, in the intervention group. These are important results particularly given the demographic profile of the participants and evidence of population level inequalities in child oral health in relation to social disadvantage and family migrant background, indicating the promise of the Teeth Tales intervention model.
2. Impact of research on health policy or professional practice
The participatory approach of the study has ensured community, service provider and government input at all stages of the study design, implementation, interpretation of results, and dissemination of findings and resources. There have been multiple impacts on policy and practice at State government, local government, cultural and community organisation levels due to the findings from the Teeth Tales study.
- Experienced oral health peer educators are now working in Victoria Arabic Social Services and Arabic Welfare
- The dental service model for Merri Community Health Services now includes a community outreach and child oral screening component (called Little Smiles)
- The Teeth Tales child oral health education manual is managed and distributed by Merri Community Health Services to other interested community organisations, with train-the-trainer support. It can be accessed from the MCHS website here
- Teeth Tales findings are directly informing Dental Health Services Victoria child oral health clinical guidelines
- Teeth Tales peer educators were employed by Merri Community Health Services as community workers.
- - Publication in 2014 and ongoing provision of the Teeth Tales Cultural Competence Organisational Review (CORe) manual and resources is managed by the Centre for Culture, Ethnicity and Health (CEH) as a free resource with additional training and facilitation services available on a fee for service basis
3. Impact of research on knowledge
This study makes important contributions to the limited evidence base in relation to oral health issues for families with a migrant background, including:
- Children from families with migrant backgrounds are at risk of poor oral health
- Migrant women face significant barriers in accessing mainstream dental services
- There are sociocultural differences in relation to child oral health knowledge, beliefs and practices
- Community-based oral health screening is an important means of reaching children in need of dental treatment
- Working in partnership with established cultural organisations is critical to health promotion initiatives targeting families with migrant and refugee backgrounds
- Study designs need to accommodate the spread of cultural networks versus the limited geographical boundaries of most health services
- Discussion of traditional oral health practices needs to be incorporated into oral health promotion initiatives and oral health care discussions in the clinical context
- Dental service use by migrant pre-school children is very low. The relationship between parent perception of their child's need to dental treatment, children's actual treatment needs, and dental service use is currently not aligned.
- Parent's length of residence in Australia, consumption of sweet drinks and parent education are predictors of child caries experience. Adding sugar to drinks is an additional risk factor for cavitation.
4. Challenges
Recruitment and retention of participants was a challenge in this study. It was particularly challenging for the Pakistani peer educator group, who were not part of an existing ethno-specific agency. This was mainly due to the difficulty of identifying eligible families without an existing client base and network. The model for intervention delivery could be developed further to align more closely with existing community and social groups, events and services to encourage uptake of the intervention.
Acknowledgements
We thank the generous contribution of families and participating organisations to this study. We also acknowledge the support of the Department of Education and Training.
Research Team
 A/Prof Lisa Gibbs, Jack Brockhoff Child Health & Wellbeing Program
A/Prof Lisa Gibbs, Jack Brockhoff Child Health & Wellbeing Program Vale Prof Elizabeth Waters, Jack Brockhoff Child Health & Wellbeing Program
Vale Prof Elizabeth Waters, Jack Brockhoff Child Health & Wellbeing Program- Associate Professor Andrea de Silva, Dental Health Services Victoria
- Dr Mark Gussy, La Trobe University
- Ms Lisa Gold, Deakin University
- Professor Laurence Moore, University of Glasgow
- Professor Richard Watt, University College London
- Dr Christine Armit, Menzies School of Health Research
- Adjunct Professor Hanny Calache, Dental Health Services Victoria
- Dr Elisha Riggs, Murdoch Children's Research Institute
- Ms Maryanne Tadic, Merri Community Health Services
- Dr Bradley Christian, Jack Brockhoff Child Health & Wellbeing Program
 Dana Young, Jack Brockhoff Child Health & Wellbeing Program
Dana Young, Jack Brockhoff Child Health & Wellbeing Program- Mandy Truong, Jack Brockhoff Child Health & Wellbeing Program
Funding Source
This project was funded by an Australian Research Council Linkage grant (LP100100223), with cash and in-kind contributions from Linkage partners—Merri Community Health Services, Dental Health Services Victoria, Moreland City Council, Victorian Arabic Social Services, Arabic Welfare and Pakistan Australia Association Melbourne. Additional funding support was also provided by Merri Community Health Services. Separate funding grants contributing to the overall research activities were also received from Dental Health Services Victoria and Moreland City Council. Salary support from the Jack Brockhoff Foundation for Lisa Gibbs and Elizabeth Waters is also gratefully acknowledged.