EIS at the Lung Cancer Screening Symposium – May 2025
Just 39 days ahead of the national launch of Australia’s first-ever Lung Cancer Screening Program – and on the same day the World Health Assembly adopted a landmark resolution on integrated lung health – more than 250 people gathered on the traditional lands of the Wurundjeri Woi-wurrung people in Melbourne for the Victorian Comprehensive Cancer Centre (VCCC) Alliance’s Lung Cancer Screening Symposium: Setting the stage: Preparing for the 2025 lung cancer screening program national rollout.
The Evaluation and Implementation Science (EIS) Unit, part of the Centre for Health Policy at the University of Melbourne, was strongly represented at the event held on Friday 23 May. EIS attendees included A/Prof Nicole Rankin (Symposium Chair), Rebecca Zosel, Dr Dzenana Kartel, Georgia Barlett, Raya Lantin, Tescha Nicholls, and Beth Ivimey OAM.
The symposium brought together health professionals, policymakers, researchers, and consumer advocates to prepare for the program’s rollout in July 2025. It featured a dynamic and engaging agenda packed with expert presentations, panel discussions, and practical tools to support health workforce, service, and system readiness.
Harnessing implementation science
A/Prof Nicole Rankin, Project Lead of the University of Melbourne-led team that developed the National Lung Cancer Screening Program Guidelines, provided an overview of the evidence and guidelines for lung cancer screening. A/Prof Rankin took the audience on a whistle-stop tour of the evolution of lung cancer screening research, highlighting the critical role of implementation strategies: methods or techniques used to enhance the adoption, implementation and sustainability of an intervention in practice.
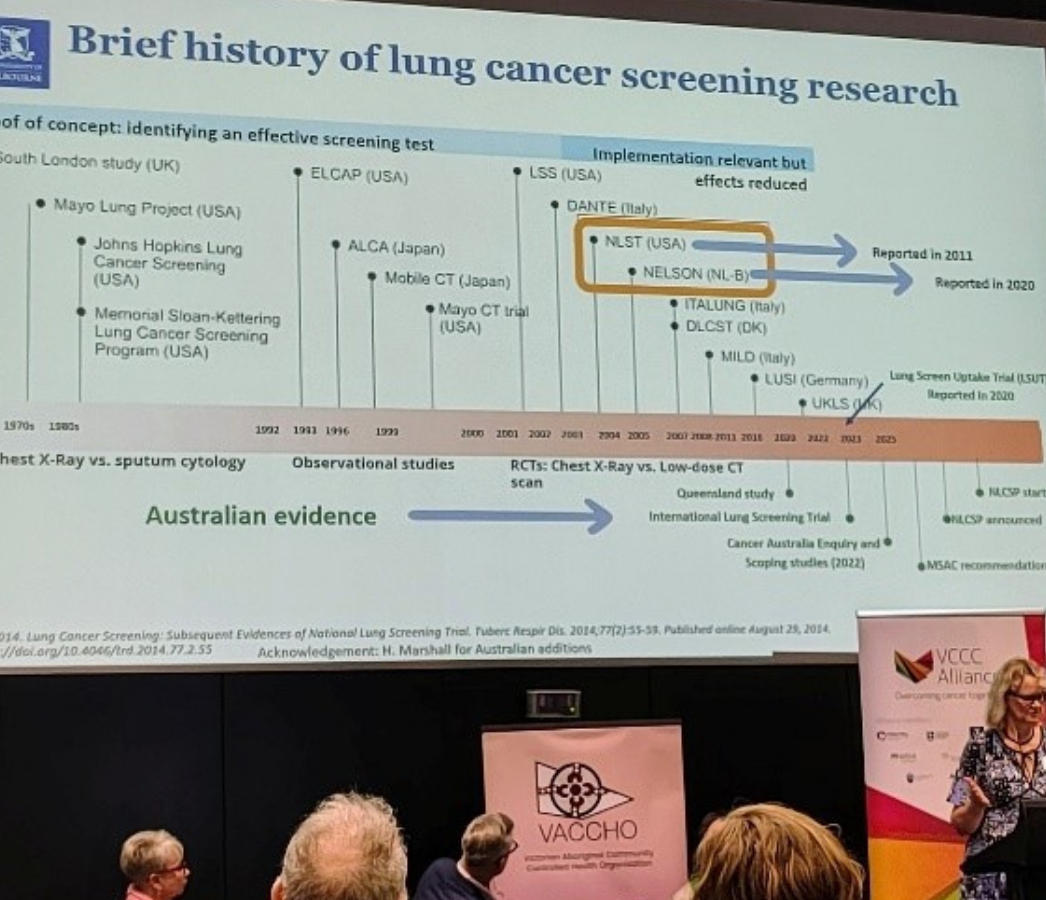
A/Prof Rankin examined the lung cancer screening program within the continuum of implementation research (World Health Organization, 2013), noting that research questions and activities become more implementation-intensive as we move downstream, beyond establishing efficacy and effectiveness. In Australia, implementation research is now the primary focus of the lung cancer screening program, as the country moves toward program rollout. The emphasis is on informing scale-up, health system integration and sustainability, and on measuring implementation outcomes such as acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, coverage, and long-term sustainability.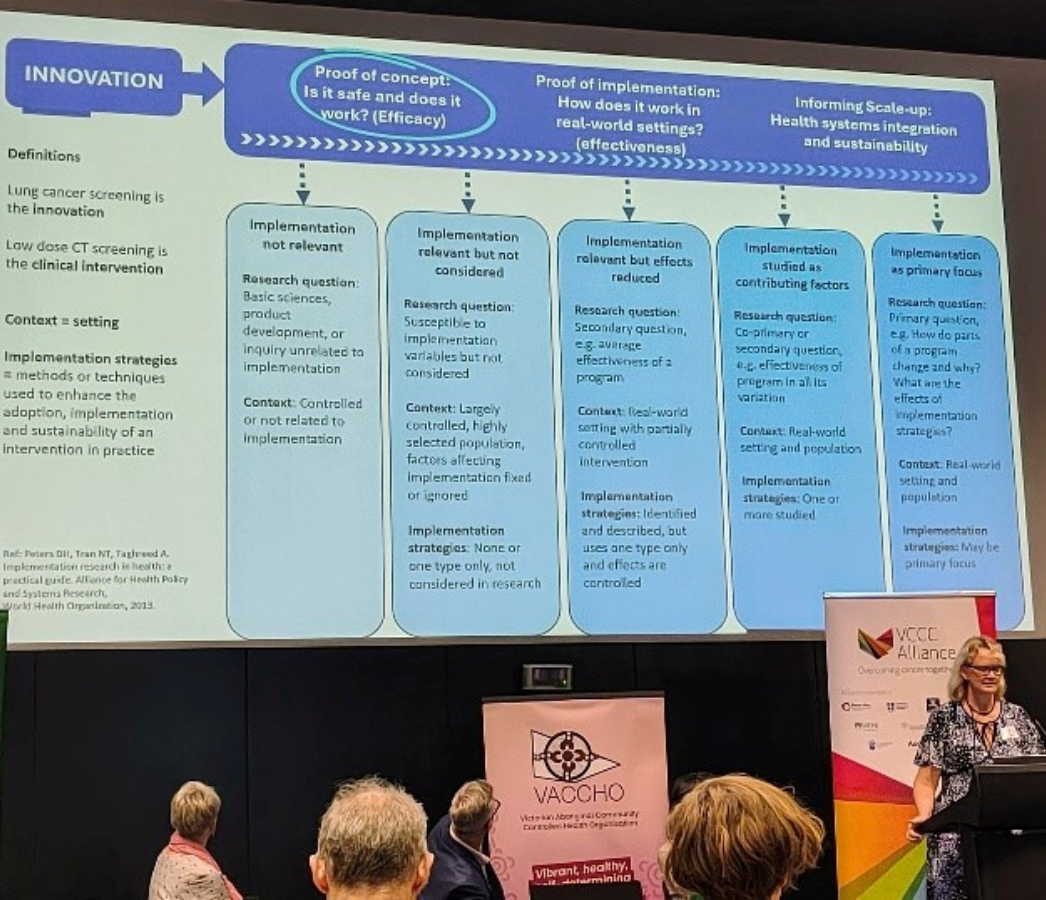
The National Lung Cancer Screening Program Guidelines provide evidence-based recommendations and practice points to support the standardised delivery of the program within the Australian setting. Ongoing monitoring and evaluation will be critical to ensure the program remains fit-for-purpose and true to its values – being agile, research and data driven, and evidence-based.
Smoking cessation and health equity
A consistent theme across the symposium was the essential role of smoking cessation within the lung cancer screening program. There was strong consensus that cessation support must be a core, integrated component of the program—not optional, but a shared responsibility among all healthcare providers. This aligns with the smoking cessation recommendations in the National Lung Cancer Screening Program Guidelines.
National Lung Cancer Screening Program Guidelines Recommendations for Smoking cessation
- All people who currently smoke or have recently quit should be offered support to quit smoking or maintain cessation using the 3-step brief intervention model – Ask, Advise, Help.
- Referral to telephone call-back counselling services can be offered to all people who smoke (where appropriate).
- Smoking cessation supports are to be offered to all potential participants by healthcare providers across the screening and assessment pathway. This includes follow-up and maintenance support.
- Offer follow-up support to all people who are attempting to quit smoking.
A/Prof Henry Marshall reinforced this by noting:
- Around 95% of screening participants won’t have lung cancer - the greatest benefit of the Program may come from quitting smoking.
- An opt-out model for cessation support can double quit rates.
- Failing to identify and treat tobacco use is not only negligent but also breaches principles of justice and exacerbates health inequalities.
A/Prof Cathy Segan from Cancer Council Victoria added that asking about smoking, when done respectfully, does not damage rapport. In fact, patients referred by a healthcare provider are 13 times more likely to quit.
Consumer advocate Anne Fidler shared her lived experience of stigma as a person with a history of tobacco use, offering practical suggestions for reducing stigma in lung cancer screening communications.

Speakers also reiterated a sobering truth: tobacco is highly addictive and remains the leading preventable risk factor for lung cancer. As one noted, we sell a product that, when used as intended, kills—let’s not forget that this is why we need a lung cancer screening program.
Equity alone is not the destination
The symposium featured a dedicated session to approaches for Aboriginal and Torres Strait Islander peoples, who are more than twice as likely to be diagnosed with lung cancer – and 1.8 times as likely to die from the disease – than non-Indigenous Australians. See the VCCC Alliance event wrap: Ensure lung cancer screening is delivered equitably, is culturally safe.
A/Prof Kalinda Griffiths delivered a powerful presentation on Indigenous data sovereignty, urging attendees to flip the model—from burden to empowerment, and from equity to sovereignty.
 She challenged the audience to move beyond conventional interpretations of equity in healthcare, emphasising that equity alone is not the destination. Rather, it is a necessary step toward sovereignty—where Aboriginal and Torres Strait Islander peoples lead, own, and determine the policies and programs that impact their health and wellbeing.
She challenged the audience to move beyond conventional interpretations of equity in healthcare, emphasising that equity alone is not the destination. Rather, it is a necessary step toward sovereignty—where Aboriginal and Torres Strait Islander peoples lead, own, and determine the policies and programs that impact their health and wellbeing.
A/Prof Griffiths stressed the importance of embedding equity at every stage of the lung cancer screening pathway—from program design and implementation to monitoring and evaluation. This must go beyond consultation to ensure Aboriginal and Torres Strait Islander leadership at all levels, where Indigenous voices and knowledges shape the program’s direction.
She also highlighted ongoing challenges with measuring Aboriginal and Torres Strait Islander cancer outcomes. She reminded the audience that data is not neutral – how it is collected, interpreted, and used reflects broader societal values and power structures. A/Prof Griffiths called for a stronger focus on measuring what matters, ensuring that data – both numerical and narrative – is relevant, meaningful, and returned to communities. This not only makes inequities visible but also empowers communities to take informed action.

A critical message was the need to move beyond counting to being accountable. Tracking participation rates or outcomes is not enough. There must be a commitment to measure what matters, collect complete, high-quality and accurate data, and to take meaningful action to address systemic barriers and uphold the rights and agency of Indigenous peoples.
This focus is especially important as the lung cancer screening program moves toward implementation. It aligns with the Medical Services Advisory Committee (MSAC) recommendation to review the program in five years, ensuring it delivers clinical effectiveness, safety and cost-effectiveness.
- Visit the VCCC Alliance website to view the symposium program.
- Visit the Australian Government Department of Health, Disability and Ageing National Lung Cancer Screening Program website.
Article prepared by Rebecca Zosel.